Using light and darkness as treatment (less med’s!)
Much of the information on this page is new research, not yet repeated by other scientists (it is always a good sign in this business if someone can repeat the study and get the same results!). However, what you’ll read here is of great importance, because it points toward a non-medication treatment for bipolar disorder that’s cheap and easy and safe. So it seems worth presenting, even though the research in this realm is just in its beginning stages. I am proud to have made an initial contribution. Phelps, Burkhart
A colleague in Norway is conducting the first large randomized trial now. A promising case report from that study has already been published.Hendricksen
Here we’ll look at how light affects the brain; how lithium affects that same pathway; how exposure to light affects that pathway; and how we can use this knowledge as part of standard bipolar treatment.
How Light Affects the Brain
You know about rods and cones, right? Those are the two kinds of receptors in your eyeball, on your retina, for light. But you didn’t know that there is another receptor for light in the eye (I’m guessing you don’t know, because until I came across this research, I didn’t know either).
Whereas the rods and cones send information to the visual cortex (the “occipital cortex”, at the back of your head), this other light receptor sends its information to your internal clock. The nerve cables from these receptors don’t even go to the vision center at all. They go straight to the middle of your brain, to a region of the hypothalamus called the suprachiasmatic nucleus, which is well known to be the location of the biological clock for us humans. (That’s an oversimplification but the general idea is correct. For the minute details, light researchers would prefer an overview and series of articles in Nature 2005).
You know about this clock, right? Everybody has one: it’s the gizmo that is setting your biological rhythms every day — when you feel like eating, when you feel like sleeping, when you feel like getting up in the morning. It’s the gizmo that gets confused by east-west travel, causing “jet lag”. It regulates hundreds of chemical reactions all timed to match the natural cycle of days and nights in our environment.
Or what used to be our environment. Nowadays we’ve altered that environment in many ways, of course (Nature is getting ready to get back at us, big time; but hey, that’s our kids’ worry, right?). One of the most significant changes in our environment is our ability to have LIGHT when we used to have DARKNESS.
But our brains were not built for this. There were built for a regular period of darkness within every 24 hours (by whom or what doesn’t matter right now; don’t stop, read my page on evolution later. I keep interrupting you with these big-picture ideas like God and global warming. I must be worried about something). Some people are not very strongly affected by our artificially lit environment. But some people, perhaps especially those with bipolar disorder, may suffer when they get too little, or too much. Right now most such people just have to learn this the hard way. Read on.
From the retina, to the biological clock: then what?
Your biological clock resets itself every day by the appearance of morning light. That’s why you can, over a few days, adjust your clock if you fly to some other continent, or even across one. As you may know, our biological clocks are not perfect 24-hour machines. They drift a little bit every day. Most people drift toward a longer day (their clock takes morethan 24 hours to complete a cycle). This is probably why most people find it easier to stay up late than to wake up early. For some people, that drift toward later hours can be very dramatic. They may be the ones who most need to learn about what I’m presenting here. They don’t stay glued to “real time” very well. They need to avoid getting “unglued” any further. And light at night may be one of the most important ungluing factors.
So, how does the clock reset itself?
Here’s the short answer. The long answer is a beautiful example of brain science; I’ll send you there in a minute if you’re interested. Briefly then: every morning light turns off a chemical process and allows the clock process, which is a very interesting string of chemical reactions, to start all over again. Clock researchers have identified all the important molecules in this process. Lo and behold: lithium directly affects one of the key enzymes in the resetting of the clock. Here we find “ground zero” of our biological rhythms, the very center of the clock process, and there’s lithium right in the middle of it. Very interesting. If that’s enough to get you interested, have a look at the long story about how the clock works, including how lithium affects it.t
Light is central to biological rhythms — and so is DARKNESS
If light starts the clock every day, is it possible that darkness is a necessary ingredient as well? Look at the question this way: sleep deprivation can cause manic episodes. In part that’s too little sleep itself — but might part of the story be “too much light?” Generally when people are sleeping less and heading toward mania, they’re not hanging out in the dark. They’re up late at night in very well lit places, like casinos, roadways with bright car lights in their eyes, their office preparing the big talk that will secure their future millions, and so forth. They’re not sitting in some dark room. Is there any chance that being forced to stay in the dark during an emerging manic episode could actually turn them in the other direction? We’ll look at some evidence for that in just a moment.
Here’s another angle on light and dark: suppose that the appearance of light every morning can reset your clock only when you’ve had enough darkness. Maybe the brain needs to be able to see the contrast? What would happen if you didn’t get enough darkness? Maybe you’d lose your biological rhythm entirely; your body wouldn’t know when to make you sleep and when to wake you up. You’d be up in the middle of the night sometimes, for days in a row, backwards to real time. Then you might be so asleep during the real day you could hardly get out of bed; getting up in the morning would feel like getting up from sleep in the middle of the night does for the rest of us, ugh.
And finally, imagine that if your clock cuts loose from real time, you lose even the 24-hour connection. Remember, the clock is not really a 24 hour machine in most people. Maybe you would lose your rhythm entirely so that you body could do the sleep thing, or the really awake thing, at any time, on any day. You’d have no idea where you were, in terms of body cycling, totally erratic. Extreme forms of “rapid cycling bipolar disorder” look just like this: no rhythm at all.
All of these lines of thought led a research team at the National Institute of Mental Health to wonder: maybe some people with rapid-cycling bipolar disorder have lost the connection between their internal clock and external light/dark reality. Maybe one way to treat that would be to simply “enforce darkness”! The results of their test of this idea will be described in a moment.
Treatment Implications
There are two aspects of this story with major implications for treatment of bipolar disorder: first, sleep and rhythm; and then, darkness and light (particularly one kind of light).
Sleep and Rhythm
This one’s pretty simple. Everybody needs sleep. But people with bipolar disorder need to protect it. Sleep deprivation is associated with having manic symptoms. But perhaps even more important than sleep, or at least as important, is rhythm: the sleep needs to happen at the same time every day to keep your clock organized. Move it around too much and you may be setting yourself up for cycling, perhaps even the harder to treat version, “rapid cycling”.
Thus most people with bipolar disorder will not be able to do “shift work”, where the work day is rotating around the clock. That’s probably about the worst kind of job schedule you could arrange. A close second worst is might be an international job like pilot or flight attendant, changing time zones over and over again. Third worst would be graveyard shift work, unless you were extremely attentive to keeping your light exposure limited to your “day”, and avoiding real daylight during your “night” (heavy blinds and a sleep mask, for example). Even then we might wonder if there’s something about “real” daylight that’s important to synchronize with your internal clock.
So, the treatment bottom line: have regular sleep hours — even on weekends. I know, it’s going to feel really stupid to be getting up at 6 am on a Saturday. You’ll probably have to conduct some personal tests to find out if this is really worth it. I’ll admit: even if it’s theoretically a good idea for the long run, you’ll probably never be able to keep it up unless you discover some shorter-term benefit as well. So keep some mood/energy/sleep records and see what you think.
Darkness and Light
The following recommendations are not standard. You won’t hear these from your doctor, for a while yet, anyway. They are just my opinions, some logical extensions from our existing knowledge. But since they are easy and safe, I don’t have to worry too much about being right! You can try one, or several, and see what you think.
In my opinion, everything you just finished reading suggests that if you have bipolar disorder, you should very deliberately manage your exposure to light and darkness, especially darkness. I think this may be as important for some people with bipolar disorder as regular sleep. Obviously the easiest way to arrange this would be to make sure you’re getting good quality darkness when you’re asleep. That means no nightlights (in one study, as little as 1/500th of midday sunlight, just 200 lux, was enough to disturb people’s melatonin, the sleep chemical in our brainHallam). That means don’t turn on the lights in the middle of the night if you get up to go to the bathroom (no hallway nightlight either). Don’t let early morning sun, in the summer, hit your closed eyelids (which means using, if you have to, a $3.50 sleep mask you can buy at the pharmacy. You’ll get used to it. Older guys who have to get up to urinate anyway can put it on before going back to sleep in the middle of the night).
Here a stunning case example to demonstrate how powerful “Dark Therapy” can be: a patient with severe rapid-cycling bipolar disorder who stopped cycling entirely — with no medications — just by carefully using very regular darkness (first 14 hrs a night, then within a few weeks, to stay well, only 10 hrs. a night). The graphs of his mood chart, before and after this treatment, are amazing. Please have a look, now or later, on my page about Dark Therapy.
No nightlights? (35% of new mothers use them; not good. Of course, the cell phone is worse: 59% ! McBean ) You can use nightlights, actually, but they have to emit no blue light, as you’ll see in the next section.
Alert, Alert: watch out for blue light at night.
Recent research has shown that one particular kind of light is the key to regulating the biological clock: blue light. The bottom line: blue light is a powerful signal telling your brain “it’s morning time, wake up!” For an explanation of that research, see Why Blue Light is So Important. The last thing you’d want to be doing right before bed is looking at a blue light. Uh, oh. You can see it coming, can’t you: what color is the light from your television? How about from the computer screen you’re staring at right now? (not after 9 pm, is it? uh oh…)
The good news is this: you might be able to significantly regulate your bipolar cycling, and at least find it easier to go to sleep at night (without medications like zolpidem (Ambien), lorazepam (Ativan), trazodone, etc.), by avoiding blue light at night. So, here’s the treatment recommendation doctors ought to be giving you (if they had the time to read the recent research in this area, which few do): no TV or computer after 9 pm if you’re going to bed at 10 or 11. End the TV/computer even earlier if you go to bed earlier. I’ve had quite a few patients tell me this step alone really helped them. If you took the link above to the story about the guy whose rapid cycling was treated with “Dark Therapy” and no medications, you can see how closely this recommendation matches that treatment.
A related step, recommended by Dr. Dave Avery, the light researcher at the University of Washington: get dimmers on all the lights you use after 9 pm and start turning them down around that time. In particular, avoid going in to brush your teeth at 10 pm and turning on the shaving lights! It’s just the wrong message to be sending your brain at that hour. If you have to use some sort of “night light” to guide your way to the bathroom in the middle of the night, use one that emits no blue light. Here’s a source of such nightlights.
Some people are very susceptible to light; others are not. But if you’re one who is, these could be very important ideas to consider. One woman wrote, after reading this section:
“My daughter was very recently diagnosed with Bipolar II. I found your site while trying to understand what she is dealing with. When I read the article about darkness, I was amazed. My own sleep patterns are poor at best, so I decided to try some of your suggestions. I got away from the computer and the television two hours before retiring for the night. I bought an eye mask. In a little over a week, I have gone from waking up 3 to 5 times a night (and not falling back to sleep) and getting out of bed to awaking once to turn over and fall right back to sleep! I am at the point where I am telling anyone who will listen to me.”
Yellow Eyeglasses to Avoid Blue Light?
This is going to be fashionable, trust me. In fact, it may already be fashionable (I wouldn’t be the guy to ask…) At least I’m not making any money on this, so you don’t have to distrust it for that reason (as otherwise you should, of course).
This idea is not yet fully tested (multiple studies underway as of 12/2014). I wouldn’t even talk about it if it weren’t utterly safe … and kind of a neat idea! It may even be pretty cheap: $7-$10. You’ve learned here that blue light is the strongest signal telling your brain to wake up, e.g. that page on Why Blue Light is So Important. If you still don’t trust me on this — good! — here’s a health reporter describing the entire history of blue light research. Fascinating, moderately technical but still plain english: Holzman).
So, if you just had to use your computer after 9 pm; or if for some reason you just have to use your TV after 9 pm… go ahead, try to convince me…. what about putting on a pair of glasses that could block out blue light? This might make it easier to fall asleep, as the signal telling your brain “wake up!” would be blocked.
Hey, this is not as wacko an idea as it sounds. People are already using it. I’ll show you a research result in a moment, but you may find these business-related stories even more convincing: a company from the Netherlands has started making a kind of fluorescent light that can vary the amount of blue and red light through the day — including more blue in the afternoon to help you stay
awake after lunch!
An American company makes 5 different products that limit your exposure to blue light at night (no-blue bulbs, including fluorescent and LED; blue-blocking sunglasses; and a blue-blocking filter to put over your computer screen (their site iswww.lowbluelights.com , and they are really nice folks; but there is a cheaper source for their blue-blocking glasses described below). And a small American study of people with Alzheimer’s disease showed that by using early evening blue light exposure, they could keep these folks awake later into the evening, so that they didn’t fall asleep at 7 pm and then wake up in the middle of the night.JAMA
Another important study showed that blocking blue light at night really does change brain chemistry, just as one would hope. Here’s how that was done. Melatonin, a hormone associated with falling and staying asleep, is decreased by light. That fact is very well established. What’s new is that you can prevent this reduction in melatonin by blocking blue light, with a simple pair of glasses made to block that particular color of light. They let everything else through. Things look pretty yellow through these things, but to your brain, it’s like darkness! What a trick. This crucial article, which shows that a simple maneuver like wearing a pair of weird glasses really can protect your sleep hormones, was published in 2005.Kayumov
The next step in this research will be a “randomized trial” in which some people with sleep problems are given either the amber lenses or a similar “control” lens that does not block blue light. Two small pilot-studies leading toward just such a large-scale test have been published Burkhart, Sasseville; in both reports, results suggest that amber lenses do indeed improve sleep.
Where can I buy the yellow eyeglasses?
All you need to try this idea is a pair of glasses with yellow lenses that will block blue wavelengths. Careful, however: you need 100% blockade of the blue wavelength, while allowing all of the other wavelengths to be transmitted. Typical “blue blockers”, widely available on the Internet for about $10, only block a fraction of blue light. So far, I know of two sources of lenses that block >90% of blue light. You can go to the original source, www.lowbluelights.com. Their amber lenses are about $50. But…
Here is another approach. A Corvallis sleep specialist found a way to get the same lenses for $7, instead of $50. A company called UVEX, which makes ski goggles, also makes safety lenses for all sorts of purposes. They have just the right lens tint in a pair of safety glasses for welders, sold in places like Airgas.
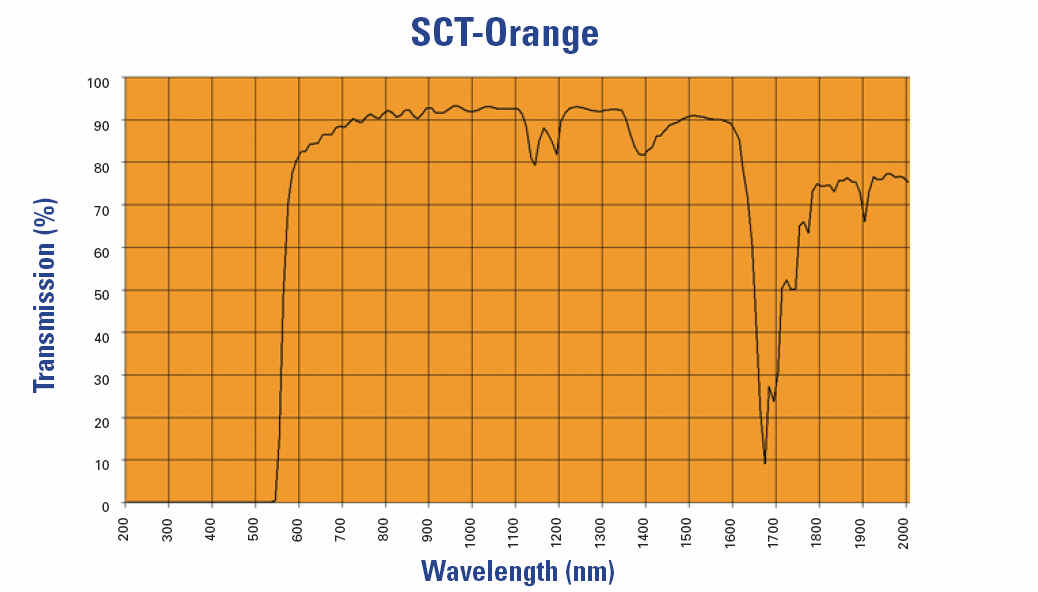
If you do not wear corrective lenses, you can use the SKYPER in the SCT Orange lens, model # 3S1933X. If you wear corrective lenses (eyeglasses), here’s a pair of amber lenses that seem to fit over my glasses quite well: the Ultraspec 2000 in the SCT Orange lens, model # S0360X. If you do not live in Corvallis: Amazon has them (they have everything?): the Skyper and the Ultraspec 2000 that fits over your glasses if needed.
If you live in Corvallis: Both models are usually in stock at Airgas, 405 NE Circle, across from McGrath’s, behind Main Auto Repair (a little tricky, look closely, they are there). Ask very specifically for the model that you need. Each are about $7.
Update 4/2010: don’t buy the cheaper Airgas-sold Radnor sport glasses with amber lenses. They look cool and they only cost $2.19, but the tint is not deep enough, so they won’t block enough blue for our purposes here. Update 10/2011: Not the Readers Digest version either.
Avoiding blue without wearing funny glasses
So far it looks like about 50% of people who wear the glasses see a clear improvement in ability to fall asleep. But almost no one keeps using them, they’re such a pain. So, if you’re one of those responders, here are three simpler options.
- Just buy a no-blue lamp and use that before bed (and during the night if you’re awake and get up — like you’re supposed to– to read a dull book). Here’s a pretty one: Somnilight. If you would like a substantial discount, write me and I’ll give you the code (my non-expert attempt to measure how many people are reading this and actually planning to buy this thing. But I have no financial connection to sales of this light. I just like the guy who makes it, he’s learned a ton about all this and taught me some too).
- Same idea but cheaper: take an old lamp and put a $5 no-blue bulb in it. But wait, there’s a hitch. That’s another story.
- At least you can try to lower the amount of blue coming out of your computer, table and phone. That’s the next chapter…
F.lux, a computer program to shift light
If light matters so much, and blue light matters most regarding mood and sleep — how about just taking out the blue at night automatically? Perfect. Someone built a program for this(the f.lux program). Great. It doesn’t take out all the blue but about 98% of it based on their calculations (see their F.luxometer page and explanations). Here are details on why it won’t take out all the blue.
For complete blue-blockinng, there is a blue-blocking filter to put over your computer screen or flat screen TV from lowbluelights.com ; they also make one for iPad mini, and iPhone.
Light Therapies: dawn simulators, light boxes
Finally, what about light? A regular rhythm of light in the morning would be good, by this analysis. How are you going to arrange that? Here we’ve left the realm of good solid research. So you don’t have to go buy one of these, just think about it: what about a “dawn simulator” for use when the sun is coming up long after your alarm? This is not a light box. It costs about $100. It’s just a light next to your bed that gradually comes on over about 45 minutes, while you’re asleep. Your regular bedside lamps can be part of it. The light will go through your eyelid and your brain will see it, even though your eyes are still closed (remember that special light receptor that connects straight to your biological clock; it works with eyelids closed!) You probably won’t need it in the summer; but depending on how far North you live, you might need it in the winter to have a more summer-like light exposure in the morning. (Here’s a list of dawn simulators by price and options).
Then there’s a true “light box”. These used to be big, suitcase-sized boxes, very bright, hard to tote around, and hard to situate near your breakfast table or bed (we’re talking morning light, right?). But now there’s a tiny one, about the size of your hand, the “little blue one”. If you’re not almost asleep already, and you’re interested in light as therapy, learn whyblue light is so important. Consider a light box if you have repeated winter sag in mood and energy. Here’s the full story on light therapy.
Conclusion
May I emphasize DARKNESS as the potential unsung friend of people with bipolar disorder. Of all the things you could do for yourself to minimize the number of medications you take, and get the best possible outcome, this could be the easiest and it is almost certainly the safest (you can’t even twist your ankle with this approach!). Regularly timed, light-free darkness is your friend.
If you’re going to use light therapy, learn about the why blue light may be the key. Then learn about light therapy in general.
Now gloat, because you know a lot about light and dark that many people with bipolar disorder don’t!
If you would like to read a 4 page summary of blue light research by a health reporter, try this one: Holzman (same link as above; moderately difficult but still plain English).
Related pages
So that you don’t have to chase them down if you skipped a link you’d now like to pursue, here are those which have been presented in this essay:
Technical Details
In case someone needs the transmission data for the UVEX amber lenses, here ’tis:

And then you’d need to know that 550 nm light, where the graph line shoots up indicating that wavelength is “greener” is being transmitted, does not affect the circadian system much. Well, that’s not perfect. If the light is bright enough, it will, and if you are exposed long enough. But that green light is surely less powerful in this respect compared to blue light, as shown in this graph (I’m saving this information for myself. If you understand it, great. If not, well, you weren’t expected to show up here! You’re welcome of course. If necessary, you’ll figure out what these graphs mean:)